Most people who’ve been told they have atherosclerosis, elevated cardiovascular risk, or “hardening of the arteries” get the same conversation: lower your LDL, take your statin, change your diet. That advice is supported by long-standing clinical evidence. But it addresses one layer of a problem that runs considerably deeper.
Atherosclerosis involves inflammation, vascular damage, and disrupted lipid metabolism.
Standard treatments are excellent at managing risk factors and preventing acute events. What they don’t target, at least not directly, is the membrane-level lipid environment.
This is where Plaquex therapy is intended to act. Not as a replacement for statin therapy or standard cardiovascular care, but as an approach that targets a different biological layer of the same underlying disease process.
This article compares how conventional atherosclerosis treatments and Plaquex IV therapy work, what each is intended to accomplish, and what the research actually says about each approach. The goal is to clarify how these approaches differ so patients can have better-informed conversations with their providers.
How Atherosclerosis Develops
The process starts with endothelial damage: something, whether it’s oxidized LDL, inflammatory signaling, or mechanical stress, disrupts the thin inner lining of an artery. LDL particles infiltrate the vessel wall, get oxidized, and trigger an immune response. Macrophages try to clean up the mess, become engorged with lipids, and transform into foam cells. Over years and decades, this accumulates into a plaque.
Growing plaques can narrow the artery enough to reduce blood flow to the heart, brain, or limbs. More immediately dangerous is when a plaque ruptures. The exposed lipid core triggers rapid clot formation, blocking the artery entirely. That’s the mechanism behind most heart attacks and strokes.
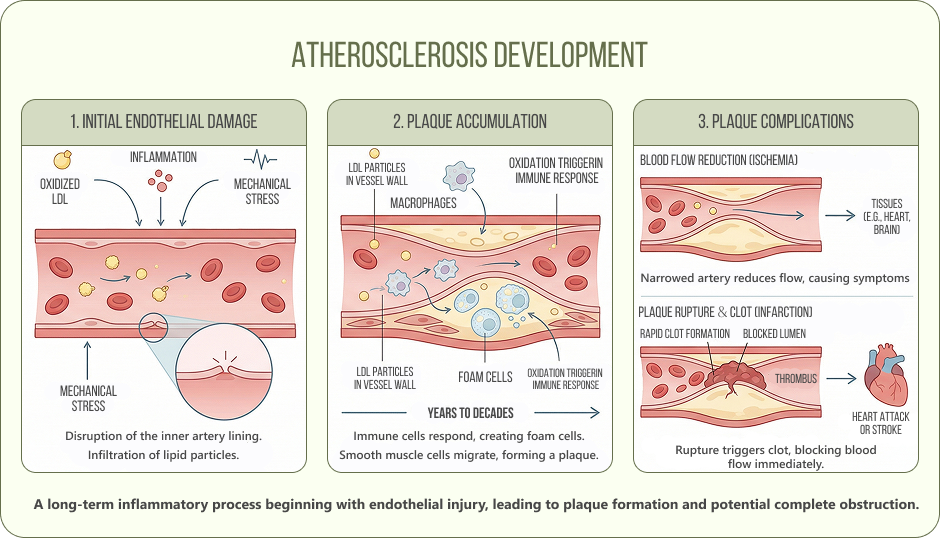
Managing atherosclerosis means addressing lipid levels, inflammation, clot risk, and the integrity of the vessel wall itself. No single therapy covers all of this, which is why combination approaches are the clinical norm.
Conventional Treatments: What They Target and How
Statins and LDL Reduction
Statins inhibit HMG-CoA reductase, the liver enzyme responsible for cholesterol synthesis. Less cholesterol produced in the liver means less LDL circulating in the bloodstream, less infiltrating arterial walls, and, over time, slower plaque progression. They also have anti-inflammatory and plaque-stabilizing effects beyond their lipid-lowering action.
A 2025 meta-analysis published in Atherosclerosis analyzed 66 studies across 3.3 million patients and found that good adherence to statin therapy reduced all-cause mortality by 35%, cardiovascular events by 24%, myocardial infarction by 30%, and stroke by 32%. That’s a level of evidence most therapies never reach. Statins work, consistently, across primary and secondary prevention, and at scale.
On the imaging side, a landmark NEJM trial by Nissen et al. used serial intravascular ultrasound in 1,039 patients and found that intensive statin therapy produced measurable regression of coronary atherosclerosis in the majority of treated patients over two years. Not just slowing the disease, actual regression. That’s the kind of endpoint most clinicians look for.
Antiplatelet Therapy
Aspirin and clopidogrel reduce platelet aggregation, lowering the risk of clot formation when a plaque ruptures. They don’t change the plaque itself or reduce LDL. Their role is specifically about preventing the acute event, the moment when a ruptured plaque triggers a heart attack or stroke.
NAC contributes to many important biological processes:
Lifestyle Interventions
Diet, physical activity, smoking cessation, and weight management address multiple risk pathways simultaneously:
- Reduce LDL and triglycerides, raise HDL
- Lower systemic inflammation
- Improve endothelial function and blood pressure
- Reduce insulin resistance, which accelerates atherogenesis
No medication fully substitutes for these. Lifestyle interventions are foundational, not optional extras.
Interventional Procedures
When arterial narrowing is severe or an acute event has occurred, percutaneous coronary intervention or bypass surgery mechanically restore blood flow. These address the downstream consequence of atherosclerosis rather than the underlying disease process.
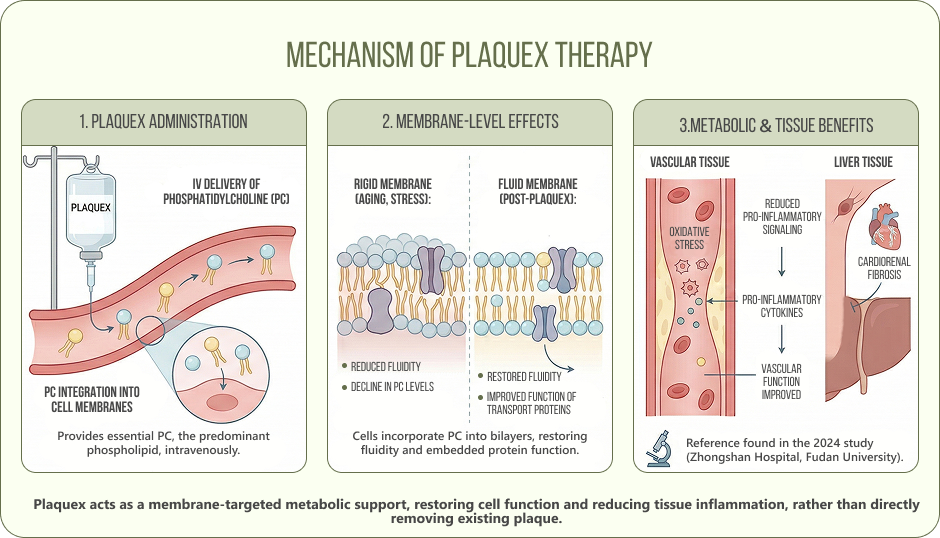
How Plaquex Works: Mechanism of Plaquex Therapy
Plaquex delivers polyunsaturated phosphatidylcholine (PC) intravenously. PC is the predominant phospholipid in mammalian cell membranes.
When phosphatidylcholine levels in cell membranes decline, as they do with aging, metabolic stress, and chronic inflammation, membranes become more rigid. In the context of cardiovascular and metabolic health, this matters in specific ways.
PC delivered via Plaquex is taken up by cells and incorporated into membrane bilayers. In experimental models, this has been shown to:
- Restore membrane fluidity in endothelial and hepatic cells, improving the function of membrane-embedded lipid transport proteins
- Reduce oxidative stress and pro-inflammatory cytokine production in vascular and liver tissue
A 2024 experimental study from Zhongshan Hospital, Fudan University, published in Frontiers in Cardiovascular Medicine found that polyenylphosphatidylcholine reduced cardiorenal fibrosis and improved vascular function in hypertensive rats through anti-inflammatory and antioxidant signaling pathways. This is animal data, so it doesn’t translate directly to clinical practice, but it adds mechanistic support for the idea that PC has measurable effects on vascular tissue beyond simply altering lipid levels.
What Plaquex is not: it doesn’t inhibit cholesterol synthesis, it doesn’t prevent platelet aggregation, and it isn’t an artery-clearing or plaque-dissolving therapy. Those descriptions misrepresent the mechanism. Plaquex IV therapy for atherosclerosis and heart disease is used clinically as a membrane-targeted, metabolic support intervention, not as a cardiovascular treatment in the conventional pharmacological sense.
Plaquex vs Statins: Comparing Mechanisms and Goals
The table below compares the primary mechanisms and clinical goals of each approach. This is an educational comparison, not a ranking of effectiveness.
|
Conventional Treatments |
Plaquex (PC Therapy) |
| Primary target |
Cholesterol synthesis, platelet aggregation, systemic risk factors |
Membrane phospholipid composition, cellular lipid transport |
| Mechanism |
Inhibit cholesterol synthesis (statins); reduce clot risk (antiplatelets); address risk factors (lifestyle) |
Incorporate into cell membranes; may support lipoprotein metabolism, LCAT activity, and inflammatory signaling |
| Biological layer |
Systemic: circulating lipids, clot risk, risk factor burden |
Cellular: membrane fluidity, lipid transport protein function, hepatic lipid handling |
| Clinical goal |
Reduce cardiovascular events; lower LDL; slow or reverse plaque progression |
Support membrane-level metabolic function; explored as adjunct in cardiovascular and metabolic protocols |
| Evidence base |
Extensive: large-scale RCTs, outcome data, guideline-endorsed |
Limited: experimental models and observational data; no large-scale RCTs in cardiovascular endpoints |
| Regulatory status |
FDA-approved / guideline-recommended for atherosclerosis management |
Used as adjunctive IV therapy in integrative settings; not FDA-approved as cardiovascular treatment |
Key Differences at a Glance
- Conventional therapies target LDL cholesterol and clot risk at the systemic level
- Plaquex targets membrane-level phospholipid composition and cellular lipid processing
- The evidence base differs significantly: decades of RCT data for statins vs experimental and observational data for Plaquex
- Clinical roles are not interchangeable; Plaquex is not a substitute for prescribed cardiovascular medications
- Patients with atherosclerosis risk may benefit from addressing both biological layers as part of an individualized protocol
What This Means Clinically
The table above shows a clear divergence in biological targets. That divergence has a practical implication: these therapies don’t compete with each other because they’re not trying to do the same thing.
A patient on statin therapy is addressing circulating LDL, systemic inflammation, and event risk. Those are real, established, guideline-supported benefits. But statins don’t restore phosphatidylcholine levels in arterial or hepatic cell membranes. They don’t address the cellular-level lipid environment that may be contributing to ongoing metabolic dysfunction.
This does not diminish the role of statins, but highlights where Plaquex is discussed instead.
For patients who are already on standard cardiovascular therapy and want to address the cellular dimension alongside it, Plaquex may be worth exploring in a clinical context. For patients who are not on standard therapy and are considering Plaquex as a replacement, that conversation needs to start with their physician.
What the Research Says
The depth and quality of evidence for these two approaches differs substantially. This difference is important and should be stated clearly.
For statins:
The 2025 meta-analysis in Atherosclerosis is one of the most comprehensive adherence analyses to date. 66 studies, 3.3 million patients. What it shows is not just that statins work in controlled trials, but that the real-world benefit tracks closely with how consistently patients actually take them. If you’re prescribed a statin and you take it reliably, the data suggests meaningful reductions in mortality, heart attack, and stroke.
The NEJM imaging trial adds something different to that picture. This trial used serial intravascular ultrasound to look directly at the plaques. Two years of intensive statin therapy produced actual regression of atheroma volume in the majority of patients. That’s direct evidence of the mechanism working at the arterial wall, not just a downstream reduction in events.
For Plaquex:
The 2024 experimental study from Fudan University in Frontiers in Cardiovascular Medicine demonstrated that polyenylphosphatidylcholine reduced fibrosis and improved vascular function in hypertensive rats. But it’s a rodent model. It helps explain the mechanism, but does not establish clinical outcomes in humans.
A 2025 meta-analysis from Cureus covering 506,813 patients reinforces just how much outcome data exists for statins specifically. Plaquex has no equivalent body of human trial data targeting cardiovascular endpoints. That’s not a reason to dismiss it as an adjunctive approach, but it is a reason to be clear-eyed about what is and isn’t established.
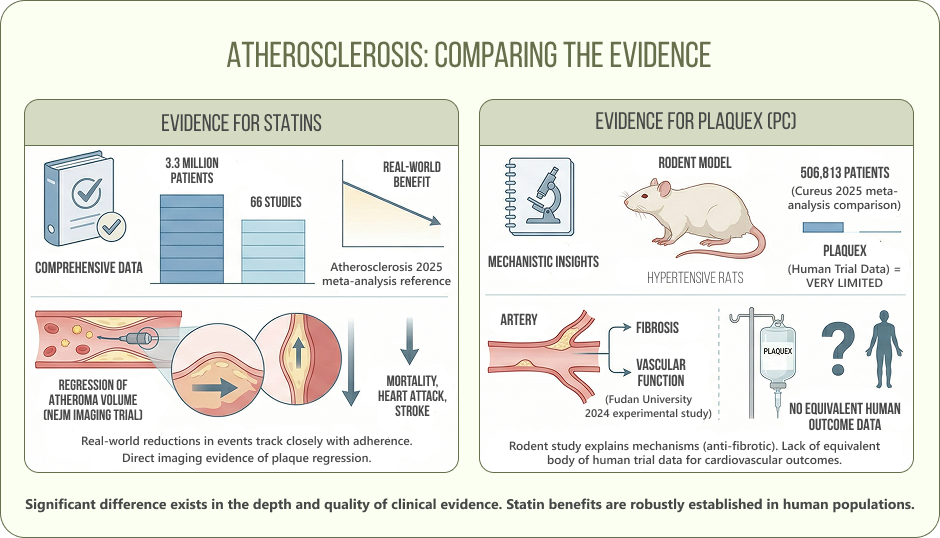
Bottom line on the evidence: statins have large-scale RCT outcome data. Plaquex has experimental and observational data supporting its membrane-level mechanism. Both approaches are grounded in real data, but differ significantly in scale and clinical evidence.
Clinical Perspective: What Patients Should Know
Plaquex is not a replacement for standard cardiovascular care. If you have diagnosed atherosclerosis, high LDL, or established cardiovascular risk, the first conversation is about statins, lifestyle, and guideline-based management. That’s the foundation. Plaquex doesn’t replace that foundation.
Where Plaquex may be relevant to discuss:
- Patients already on standard cardiovascular therapy who want to address membrane-level lipid metabolism alongside it
- Those in an integrative wellness protocol who are working with a physician on a multi-layer cardiovascular and metabolic strategy
What is not appropriate: using Plaquex as a reason to delay or discontinue prescribed cardiovascular medications. Any adjustment to a cardiovascular medication regimen needs to be made with the prescribing physician, not based on interest in adjunctive therapies.
The Invita Approach: Protocol-Based, Not Piecemeal
At Invita Wellness in NYC, Plaquex IV therapy is positioned as a cardiovascular and metabolic support therapy within a structured, physician-supervised protocol. It’s not offered as a standalone treatment or as an alternative to cardiology care. The clinical value comes from targeting the cellular layer of cardiovascular health alongside whatever systemic management a patient already has in place.
In practice, that means a protocol built around your specific metabolic profile, not a generic infusion schedule. For some patients, Plaquex is combined with NAD+ therapy to address mitochondrial energy production alongside membrane health. What stays consistent is the approach: assess first, build the protocol around the individual, and track results.
At Invita, Plaquex is not positioned as a replacement for standard care what your cardiologist prescribes. It’s that cardiovascular health involves biology that standard prescriptions don’t fully address. If you’re already managing your LDL and your clot risk and you still feel like something is being left on the table, cellular membrane function may be part of the answer.
Every protocol at Invita starts with a clinical consultation and individual assessment. A therapy that works for one patient may not be appropriate for another.
Conclusion
Conventional atherosclerosis treatments and Plaquex therapy are not in competition. They operate at different biological levels, target different aspects of the disease process, and have very different evidence bases behind them. Understanding that distinction is what allows patients to make genuinely informed decisions about their cardiovascular health strategy.
Statins reduce LDL, stabilize plaques, and prevent cardiovascular events. This is well-established in clinical guidelines and remains the foundation of care for patients with significant cardiovascular risk. Plaquex supports membrane-level lipid metabolism and cellular function. That’s a real biological target, but one backed by experimental and early-stage clinical data, not large-scale outcome trials.
If you’re managing your cardiovascular risk and want to understand whether a cellular-level intervention makes sense as part of your protocol, that’s a conversation worth having with a provider who understands both layers. Book a consultation at Invita Wellness to review your metabolic profile and explore whether phosphatidylcholine IV therapy fits into your cardiovascular health strategy.
* Please note: This article is for educational purposes only and does not constitute medical advice. Plaquex IV therapy is not an FDA-approved treatment for atherosclerosis or cardiovascular disease and should not replace prescribed medications or standard medical care. Do not adjust or discontinue any prescribed medication without consulting your physician. All IV therapies at Invita Wellness are administered under physician supervision.
Plaquex IV therapy is your health strategy
contact InVita Wellness today
Book Now
456 Broadway 2 Floor, New York, NY 10013, USA
Dr. Leon Shapiro
Medical Director & Protocol Specialist
Medically reviewed by Dr. Leon Shapiro, MD, Harvard-trained anesthesiologist with 25+ years in clinical and research settings. Supervises InVita’s IV protocols with expertise in integrative cardiovascular and metabolic wellness.
Resources
Banach, M., et al. “Adherence to statins and development of atherosclerosis-related events: a systematic review and meta-analysis.” Atherosclerosis (2025). DOI: 10.1016/j.atherosclerosis.2025.119138
https://www.sciencedirect.com/science/article/pii/S1056872725000935
Nissen, S.E., et al. “Effect of two intensive statin regimens on progression of coronary disease.” New England Journal of Medicine 365 (2011): 2078-2087. DOI: 10.1056/NEJMoa1110874
https://www.nejm.org/doi/full/10.1056/NEJMoa1110874
Zhang, Y., et al. “Polyenylphosphatidylcholine alleviates cardiorenal fibrosis, injury and dysfunction in spontaneously hypertensive rats by regulating Plpp3 signaling.” Frontiers in Cardiovascular Medicine 11 (2024): 1458173. DOI: 10.3389/fcvm.2024.1458173
https://www.frontiersin.org/journals/cardiovascular-medicine/articles/10.3389/fcvm.2024.1458173/full
Ghani Khan, K., et al. “Effect of statin therapy on clinical outcomes in patients with cardiovascular risks: a systematic review and meta-analysis.” Cureus 17.7 (2025): e88238. DOI: 10.7759/cureus.88238
https://pubmed.ncbi.nlm.nih.gov/40831859/
